Review Article
Anxiety and depression as an effect of birth order or being an only child: Results of an internet survey in Poland and Germany
Jochen Hardt1*, Lisa Weyer1, Malgorzata Dragan2 and Wilfried Laubach1
1Medical Psychology and Medical Sociology, Department of Psychosomatic Medicine and Psychotherapy, University Medicine of the Johannes Gutenberg University Mainz, Germany
2Faculty of Psychology, University of Warsaw, Warsaw, Poland
*Address for Correspondence: Dr. Jochen Hardt, Medical Psychology and Medical Sociology, Department of Psychosomatic Medicine and Psychotherapy, University Medicine of the Johannes Gutenberg University Mainz, Germany, Tel: 0049 6131 3925290; Fax: 0049 6131 3922750; Email: [email protected]; [email protected]
Dates: Submitted: 16 August 2017; Approved: 13 September 2017; Published: 14 September 2017
How to cite this article: Hardt J, Weyer L, Dragan M, Laubach W. Anxiety and depression as an effect of birth order or being an only child: Results of an internet survey in Poland and Germany. Insights Depress Anxiety. 2017; 1: 015-022. DOI: 10.29328/journal.hda.1001003
Copyright License: © 2017 Hardt J, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Body mass index; Depression; Anxiety; Partnership; Birth status

Abstract
Background: Various studies examined the effect of birth order. First born children show usually better cognitive performance than their later born siblings. Studies on emotional aspects yield heterogeneous results, sometimes in favour of first born, sometimes in favour of later born children. Studies comparing only-children with children with siblings are rare.
Method: An internet survey was performed in 508 Polish and 500 German subjects. Only-children, first born, middle born and latest born children were compared regarding body mass index, depression, anxiety and partnership.
Results: No differences among first born, middle born and latest born children were detected. Only-children reported significantly less symptoms of social phobia than first born children (z=0.50, p< 0.01).
Conclusions: Except for suicidality, the results of this study question the sense of further investment in studying effects of birth order. In contrast, examining differences between only-children vs. children having siblings seems to have the potential to yield interesting and new results. Optimally, such research would combine self-report measures with reports from others, such as parents, teachers or clinicians.
Introduction
Birth order
Effects of birth order have been widely examined and discussed. Galton [1], already examined the birth order of scientists and found that first born children were overrepresented (Galton himself was the 9th and latest child of his parents). Adler [2], draw far reaching conclusions about birth order. He focused particularly on the fact, that a first born feels for some time being the “king or queen” of the family, but loses this status when a sibling is born. A second born makes a similar experience (if a third child is borne), but it is less pronounced because she or he have had to share the parents already with the first born sibling. Just the latest born child does not make such an experience. According to Adler, first born children are more competitive and prone to neuroses than later born ones, and the youngest children shall become most prosocial. Sulloway [3], stated that first born children adopt different roles in the family than later born ones, in particular becoming more dominant and conservative, while the later borns shall rather be prone to become rebels. Modern studies confirm these classic theories only limited, and partly contradict them [1].
Physical growth and body mass index
There is widely agreement in the literature that first borns start with a lower birth weight than later borns, but then catch up e.g., [4]. Derraik et al. and Siervo et al., found that first borns BMI was larger in adulthood, however in the Derraik study [5,6]. The difference was very small (z=0.12) and the sample very large (n=26 812). Kwok et al., also found a lower birth weight in first borns compared to later borns, at age 13 the differences were non-significant [7]. Data from adulthood are not available from the Kwok study, because the sample of this longitudinal study is not grown up, yet. In 4-8 year old children, Mosli et al. [8], found that the presence of at least one younger sibling and/or having a brother was associated with a lower BMI.
Intelligence
There is solid evidence that not only first born children are more intelligent than later born ones as Galton already observed, but that there is a declining gradient in intelligence with birth order at least among the first four siblings e.g., [9]. The effects were not strong, however, between three and zero points on the standard intelligence scale (mean=100, sd=15) per birth position, corresponding to effect sizes of d-values between 0.20 and 0 [10]. Within family comparisons yield steeper gradients than between family comparisons, and the differences between first and second born children seems to be largest. There is an ongoing debate if the gradient becomes plane when number of siblings increases above 4 e.g., [11], but samples would need to be extremely large to decide this question empirically. As an explanation for the effect it is generally assumed that earlier born children receive more attention from their parents [12]. The small average differences in intelligence due to birth order make it happen that in many families the later born children are more intelligent than their earlier born ones. Such differences are well recognized by parents and siblings and predict the academic achievement of the children [13].
Personality and Behavior
In the Rohrer et al. [9] study, additionally the big five personality traits were examined – and displayed no differences among the various birth order positions. Also Sulloways rebel hypothesis was not supported when empirically investigated [14]. Prime et al. [15], examined prosocial behaviour in first born, middle born and latest born children via an experimental design. Three year old children got a transparent plastic box containing a wrapped doll, which could not be taken alone, only in cooperation with the experimenter. As Adler would have expected, in this task last born children acted more prosocial than first born ones. However, in a study on 148 children who needed dental treatment, middle borne behaved most cooperatively [16].
However, birth order or the presence of a sibling show an important difference in behavior. The risk to commit suicide is considerably lower in first borns than in later borns, [17,18]. As compared to first-borns, second-borns had a relative risk for committing suicide of 1.27, third-borns of 1.35, and fourth- or higher-borns of 1.72, while other causes of death did not display an evident or consistent birth-order pattern [19]. Koenig [20] explained this effect with bearing early responsibility particularly in the first born, but such an explanation is certainly not sufficient [21]. Particularly in families having times with adversities (e.g. mental disorder of a parent or financial hardship), the conditions for growing up in the later borns may become less optimal than for the earlier born children.
Depression and anxiety
Two newer studies contradict Adlers hypothesis and report highest rates of depression in middle borne children [22,23], with a larger difference to first born than to last born siblings. A large, but older study found the opposite, a non-significant difference with a tendency to higher depression rates in last borns [24]. Regarding anxiety, Alvi et al. [22], found lower rates in first borns compared to later borne children. Chartier et al. [25], found the same effect for social phobia, but only in males.
Only-child vs. child having siblings
Effects of being an only-child compared to being a child with siblings have been much less examined in scientific literature than birth order. There are some studies from China, where a one child rule was installed in 1979/80 leading to more than 100 million only-children in 2008 already. Additionally, some studies conducted to examine birth order included an only-child group.
Physical growth and body mass index
Mosli et al. [8,26], compared the BMI of only-children and children having siblings in 4-8 years old in low-income families in the US. It was found that only-children and last borns had a higher BMI than first and middle-borns. Factors associated with the BMI were maternal control and support.
Intelligence
Zajonc (2001), hypothesized that the intelligence of only-children should be comparable to those of first borns or even higher. However, his first data did not support this. But newer and larger studies confirm Zajoncs assumption. Kirkcaldy [27], did not find a difference between the intelligence of only-children and firstborns [28], found that only-children even excel first borns in educational achievement.
Personality and Behavior
Guo et al. [29], compared only-child and children with siblings in a school for nurses. They compared 20 variables examining character strength between the two groups and found for the scores of creativity, curiosity, zest, interpersonal wisdom, leadership and humor that results of the only-child group were significantly better than those of the non-only-child group. Qin et al. [30], compared the strength and difficulties questionnaire between twins and only-children of age 6-16. In the self-evaluation (done by children 11 or older), there were no differences at all, in the parent evaluation the only-children received higher values on the scale “difficulties with peers” than the twins. Bobbitt-Zeher et al. [31], found that the more children were in the family a subject grew up, the lower the divorce rates were in later life, i.e. about a 3% decrease for every sibling in those, whoever married.
Depression and anxiety
Both, the Qin et al. [30] and the Guo et al. [29], study included measures for depression and anxiety. No single difference was found between the only-children and the children with siblings in these two studies. However, a very large study (n=16 823) found higher values for depression in children having siblings than in only-children [32].
Summarizing the literature, some consistent differences for birth status were found. First, rates of subjects committing suicide differ substantially by birth order-an effect which would clearly be worth to exploring further in detail. Other effects were present, but small in magnitude. There is solid evidence that first born and only-children start with a lower weight, but then catch up. The only thing which remains unclear here, is if adult weight would become higher or similar to later borns or children having siblings, corrected for height. Second, no need for research regarding intelligence is needed any more, first born and only-children exhibit highest levels here, again the effect size is small. Results regarding anxiety and depression are strongly heterogeneous, some studies find differences, others not. Regarding peer relationships it seems to be the case that only-children are having more problems than children with siblings, but they do not seem to realize this themselves. Hence, the aim of the present study is to compare body mass index, two indicators of depression, two of anxiety and two of partnership among four groups: only-children, first-, second-, and last borns.
Methods
Sample
A total of 1008 subjects from Poland and Germany filled out a questionnaire online at the platform of a commercial company usually performing marketing research (http://www.linequest.de). The survey comprised about 280 items, participants received a compensation of about € 4.30 for filling out the questionnaire, what took about 30 minutes. The sample size calculation was based on a mean difference of d≥0.25 [33] between the Polish and German sample to be detected at alpha=0.01 with a power of 0.90 [sampsi: 34]. Participants were informed that the survey was about mental health and childhood in Poland and Germany. The scientific background of the study was posted on the homepage of the University of Mainz during data collection. The ethics commissions of the Landesärztekammer Rheinland-Pfalz (Nr. 837.185.07) and the University of Düsseldorf (5720) approved the project.
In Poland, the mean age of the subjects was about 39 years, and slightly more than half were female. In Germany, a gender and age stratified sample was drawn. As a result, exactly 50% of the Germans were female, and the sample is six years older than the Polish one. Most participants had a spouse or partner. In Poland, more participants were in partnerships than in Germany. Sample characteristics are displayed in table 1.
| Table 1: Sample description. | |||
| Poland | Germany | ||
| N | 508 | 500 | Test for differences |
| Gender: % female | 56.3 | 50.0 | χ²(1) = 4.02, p < 0.045 |
| Age: (sd) | 38.7 (14.4) | 44.8 (16.1) | t(1006) = 6.40, p < 0.001 |
| Familiy status (%) Married Partnership > 6 months Partnership < 6 months No partnership Other |
48.8 23.8 3.5 17.3 6.5 3.5 17.3 6.5 |
43.0 23.2 3.8 26.6 3.4 |
χ²(4) = 16.7, p < 0.002 |
| Birth status (%) Only child First born Middle born Last born |
17 40 19 25 |
26 36 12 26 |
χ²(3) = 18.8, p <0.001 |
Variables
Body mass index (BMI) was calculated as weight in kilogram divided by height in meter [2]. Both variables were assessed by asking the proband, not measured.
Out of the two indicators utilized assessing depression, one was assessing the mood of the past two weeks, one assessing if there was at least one lifetime depressive period. Also two indicators for anxiety were examined, i.e. symptoms of social phobia and symptoms of agoraphobia. All four were assessed by the symptom-check-list-27-plus [SCL-27+35]. Scales were right skewed, with values for skewness between 1 and 2.4 [kurtosis between 2.3 and 10.1, distributions of the scales are displayed in 36].
Partnership also had two indicators. First, the proportion of subjects was counted reporting a partnership lasting longer than six months. Second, only in the subgroups who reported having such a partnership, satisfaction with the partnership was assessed on a 100 mm long visual analogue scale. The scale had a skewness of -1.7 and a kurtosis of 6.0. All indicators except BMI were transformed into scores ranging from zero to one. Zero means that there were no symptoms present, one would indicate the maximal possible number of symptoms with maximal possible frequency (in satisfaction with partnership: not at all satisfied-fully satisfied).
Statistical Analysis
Linear and logistic regressions were performed. Birth status was effect coded with only-child as reference category [37]. Age, gender and country were added as potential confounders, as well as a quadratic term for age and all two-way interactions. A backward selection of significance tests was performed: first the interaction terms were removed if non-significant, then the quadratic effect for age if non-significant, then the non-significant main effects. Birth status was always kept in the model until the end. The alpha level for all statistical tests was set to 0.05 (two-tailed), no trends were reported. Calculations were performed using STATA 12 [34]. We report unadjusted means (Table 2) and in case of significant differences a graphical representation on estimated values controlling for the significant confounders (Figure 1) is presented.
| Table 2: Comparison among only-children, first, middle, and last born. | |||||||
| Only child | First born | Middle born | Last born | Test for differences | |||
| Variable | sd) | (sd) | (sd) | (sd) | |||
| BMI | 26.5 (5.6) | 26.0 (5.1) | 25.4 (4.4) | 25.4 (4.6) | F3;995 = 1.81 p < 0.14 | ||
| Depression | |||||||
| Lifetime | 0.25 (0.35) | 0.29 (0.36) | 0.25 (0.33) | 0.28 0(.34) | F3;1003 = 0.57 p < 0.63 | ||
| Current | 0.17 (0.19) | 0.19 (0.21) | 0.20 (0.20) | 0.20 (0.20) | F3;1003 = 1.26 p < 0.29 | ||
| Agoraphobia | 0.07 (0.14) | 0.09 (0.14) | 0.08 (0.14) | 0.09 (0.15) | F3;1003 = 1.27 p < 0.28 | ||
| Social phobia | 0.17 (0.19) | 0.23 (0.20) | 0.19 (0.19) | 0.21 (0.18) | F3;1001 = 5.10 p < 0.01 | ||
| Partnership: % Yes | 69 | 69 | 66 | 71 | χ²(3) = 1.92, p < .59 | ||
| Partnership satisfaction | 0.71 (0.32) | 0.75 (0.27) | 0.72 (0.30) | 0.75 (0.26) | F3;692 = 0.27 p < 0.85 | ||
| Note: DF in F-value denominator varies due to missing data and included covariates. | |||||||
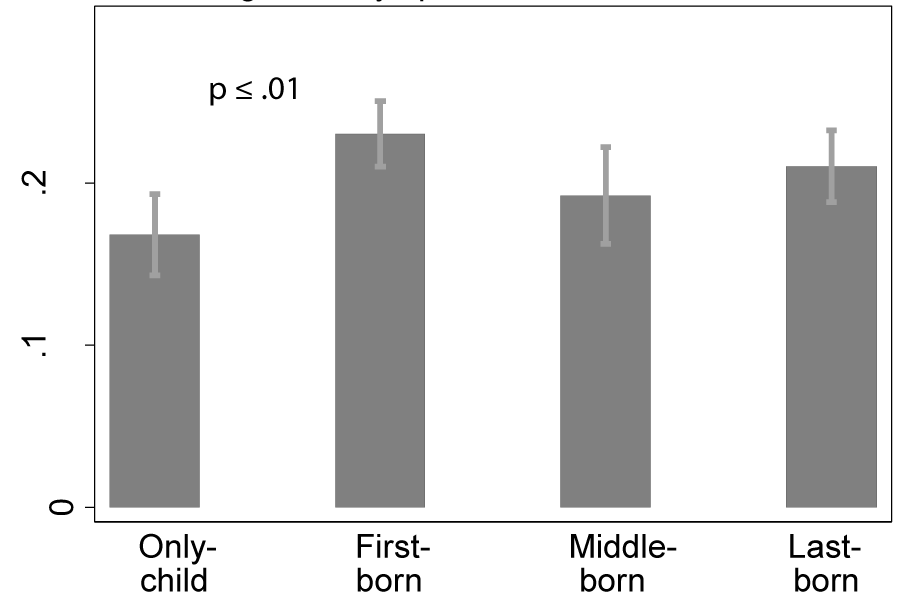
Figure 1: Estimated values for symptoms of social phobia for only-children, first-, second-and last born, controlling for age, gender and country.
Results
Polish families had a significantly lower rate of only-children than German families (17% vs. 26%, table 1). Differences among the groups of first -, middle - and last born were non-significant. Regarding the seven variables which were tested for birth status, only one effect was significant, but highly significant: Symptoms of social phobia were lower in the only-child group than in first born (Table 2, Figure 1).
Discussion
Regarding birth order, this study did not find any significant effect. No differences regarding BMI were observed in this sample of n=1000 with an average age of about 40 years. Hence, we would not criticise results from studies relying on much larger samples, but we would question their relevance for practise. As it is the case with intelligence, the effect is very likely to be present, but its size is so small, that there is not much need to focus on it. Depression, anxiety and partnership display so small differences among the birth order groups, that even much larger samples would be required to find significant differences. Given that there are substantial differences in suicidality for birth order, and depression constitutes the main predictor for it e.g., [38], such a lack of an effect for depression was quite surprising. However, we would conclude from the present results and the review of the literature that there is no need to further analysing effects of birth order, except for suicidality.
The single significant effect in this study was that symptoms of social phobia were particularly high in first born, and particularly low in only-children, middle and last born were intermediate. This results is incongruent to the one of Chartier et al. [25], who observed particularly low rates of social phobia in first born males. Differences for females were non-significant in the Chartier study. We tested such an interaction, but it proved to be nonsignificant. Additionally, the results observed here contradict the one for males in the Chartier study. One possible explanation would be that Chartier et al. used a clinical diagnosis obtained by the composite international diagnostic interview CIDI [39], and we utilized a simple questionnaire score. This implies two important differences.
(1) Chartier et al. have an objective rating, we report the subjective view of the probands.
(2) The threshold to receive a diagnosis of social phobia in the CIDI is much higher than the score of our questionnaire for most probands. Hence, in the present study mainly mild symptoms of social phobia were present, say in the sense of being shy. One or both aspects may explain the difference, but we would be cautious to say that first born have high values in symptoms of social phobia before such a result is replicated.
The other aspect of this effect, i.e. only-children report less symptoms of social phobia then children with siblings would be more plausible. Even if we could not identify any other study which examined this empirically, it would fit to the Chinese studies cited in the introduction which generally shows that only-children self-reports express a better view on themselves than those of children with siblings do. However, the results from Qin et al. [30] should be kept in mind, where parents did saw more difficulties in peer relationships in their only-children than parents of twins did, which were not reported in the self-report.
The present study has the following limitations. (1) Data rely on an internet survey. It is unknown how representative such a survey is. (2) Data are completely self-reported, no objective measurements like CIDI diagnoses were taken. (3) Compared to some other research about birth order, the present sample is relatively small. (4) Various other variables could have been chosen to examine differences among only-children, first, middle and later borns. One strength of this study shall also be mentioned. We carefully tried to partition out effects of confounders.
Given these limitations, we would conclude that research about birth order except for suicidality is no longer necessary. Birth weight and intelligence effects are sufficiently studied, and readers may decide themselves if they evaluate their effect sizes to be practically relevant or not. All other factors are likely to yield so small effect sizes, that we would suggest to say good bye to Galtons thoughts about first-borns (but not to his other work), Adler and Sulloway. To our opinion, it would be much more interesting today to further exploring differences between only-children and children with siblings-not only because there are more than 100 Millions only-children in China, but also in other countries the rate of only-children is raising. In Germany for example, 26 % of the subjects of this study, who mainly grew up in the 1960ies, were only-children, the rate of only-children in 2009 was about 34 % [40]. However, such research would optimally not solely rely on self-reports, but would integrate measures such as the view from parents, partners or clinicians assessments.
Conflicts of Interest
This work was supported, in part, by the Heigl-Stiftung, Düsseldorf and the Köhler-Stiftung, Essen (grant number 100064-06).
References
- Galton F. English men of science: Their nature and their nurture. 1874. Ref.: https://goo.gl/GsjJBv
- Adler A. Characteristics of the first, second and third child. Children. 1928; 3: 14-52.
- Sulloway FJ, Born to rebel. Birth order, family dynamics and creative lives. Ed Vintage. 1996. Ref.: https://goo.gl/h14Z3P
- Lawson DW, Mace R. Sibling configuration and childhood growth in contemporary British families. Int J Epidemiol. 2008; 37: 1408-1421. Ref.: https://goo.gl/MLeUVz
- Derraik JG, Ahlsson F, Lundgren M, Jonsson B, Cutfield WS. First-borns have greater BMI and are more likely to be overweight or obese: a study of sibling pairs among 26,812 Swedish women. J Epidemiol Community Health. 2016; 70: 78-81. Ref.: https://goo.gl/ndvisd
- Siervo M, Horta BL, Stephan BC, Victora CG, Wells JC. First-borns carry a higher metabolic risk in early adulthood: evidence from a prospective cohort study. PLoS One. 2011; 5. Ref.: https://goo.gl/UCLofY
- Kwok MK, Leung GM, Schooling CM. Associations of Birth Order with Early Adolescent Growth, Pubertal Onset, Blood Pressure and Size: Evidence from Hong Kong's "Children of 1997" Birth Cohort. PLoS One. 2016; 11. Ref.: https://goo.gl/MvuULV
- Mosli RH, Miller AL, Peterson KE, Kaciroti N, Rosenblum K, et al. Birth order and sibship composition as predictors of overweight or obesity among low-income 4- to 8-year-old children. Pediatr Obes. 2016; 11: 40-46. Ref.: https://goo.gl/grLppc
- Rohrer JM, Egloff B, Schmukle SC. Examining the effects of birth order on personality. Proc Natl Acad Sci U S A. 2015; 112: 14224-14229. Ref.: https://goo.gl/wTu4E5
- Cohen J. A power primer. Psychol Bull. 1992; 112: 155-159. Ref.: https://goo.gl/FDWjgL
- Abdel-Khalek AM, Lynn R. Intelligence, family size and birth order: Some data from Kuwait. Pers Individ Dif. 2008; 44: 1032-1038. Ref.: https://goo.gl/gY8sq2
- Zajonc RB. The family dynamics of intellectual development. Am Psychol. 2001; 56: 490-496. Ref.: https://goo.gl/YnrkFp
- Jensen AC, McHale SM. What makes siblings different? The development of sibling differences in academic achievement and interests. J Fam Psychol. 2015; 29: 469-478. Ref.: https://goo.gl/eXUEDb
- Freese J, Powell B, Steelman LC. Rebel without a cause or effect: Birth order and social attitudes. American Sociological Review. 1999; 64: 207-231. Ref.: https://goo.gl/4B9kWo
- Prime H, Plamondon A, Jenkins JM. Birth order and preschool children's cooperative abilities: A within-family analysis. Br J Dev Psychol. 2017; 35: 392-405. Ref.: https://goo.gl/pAaKsj
- Ghaderi F, Fijan S, Hamedani S. How Do Children Behave Regarding Their Birth Order in Dental Setting? J Dent (Shiraz). 2015; 16: 329-334. Ref.: https://goo.gl/uvHf9E
- Bjorngaard JH, Bjerkeset O, Vatten L, Janszky I, Gunnell D, et al. Maternal age at child birth, birth order, and suicide at a young age: a sibling comparison. Am J Epidemiol. 2013; 177: 638-644. Ref.: https://goo.gl/YN6LpG
- Rostila M, Saarela J, Kawachi I. Birth order and suicide in adulthood: evidence from Swedish population data. Am J Epidemiol. 2015; 179: 1450-1457. Ref.: https://goo.gl/kVgcEe
- Saarela J, Cederstrom A, Rostila M. Birth order and mortality in two ethno-linguistic groups: Register-based evidence from Finland. Soc Sci Med. 2016; 158: 8-13. Ref.: https://goo.gl/A2r3YW
- Koenig K. Brüder und Schwestern: Geburtenfolge als Schicksal. Vandenhook & Rupprecht. 2004.
- Rostila M, Saarela J. Invited commentary: birth order and suicide in a broader context. Am J Epidemiol. 2013; 177: 645-648. Ref.: https://goo.gl/8RTokT
- Alvi T, Assad F, Ramzan M, Khan FA. Depression, anxiety and their associated factors among medical students. J Coll Physicians Surg Pak. 2010; 20: 122-126. Ref.: https://goo.gl/hDk3tC
- Asal AR, Abdel-Fattah MM. Prevalence, symptomatology, and risk factors for depression among high school students in Saudi Arabia. Neurosciences (Riyadh). 2007; 12: 8-16. Ref.: https://goo.gl/ooH7fM
- Grosz HJ. The depression-prone and the depression-resistant sibling: a follow-up note on marital state. Br J Psychiatry. 1968; 114: 1559-1560. Ref.: https://goo.gl/AtAiXg
- Chartier MJ, Walker JR, Stein MB. Social phobia and potential childhood risk factors in a community sample. Psychol Med. 2001; 31: 307-315. Ref.: https://goo.gl/cp85Yp
- Mosli RH, Lumeng JC, Kaciroti N, Peterson KE, Rosenblum K, et al. Higher weight status of only and last-born children. Maternal feeding and child eating behaviors as underlying processes among 4-8 year olds. Appetite. 2015; 92: 167-172. Ref.: https://goo.gl/N3pB31
- Kirkcaldy B, Furnham A, Siefen G. Intelligence and birth order among children and Adolescents in Psychiatric care. School psychology international. 2009; 30: 43-55. Ref.: https://goo.gl/oKEzAq
- Travis R, Kohli V. The birth-order factor - ordinal position, social strata, and educational-achievement. J Soc Psychol. 1995; 135: 499-507. Ref.: https://goo.gl/5BCUgN
- Guo Y, Zhang J, Zhang N. Character strengths and their influencing factors among nursing students in Changsha, China: the only-child versus non-only-child. Arch Psychiatr Nurs. 2015; 29: 365-371. Ref.: https://goo.gl/pJa8zF
- Qin Q, Fu Y-X, Meng H-Q, Xiang H, Jiang J-Z, et al. Using the strengths and difficulties questionnaire to screen for child mental health in the twins and the only-child. Int J Clin Exp Med. 2016; 9: 8749-8754. Ref.: https://goo.gl/wwqeZz
- Bobbitt-Zeher D, Downey DB, Merry J. Number of Siblings During Childhood and the Likelihood of Divorce in Adulthood. J Fam Issues. 2016; 37: 2075-2094. Ref.: https://goo.gl/rnoaaw
- Carballo JJ, Garcia-Nieto R, Alvarez-Garcia R, Caro-Canizares I, Lopez-Castroman J, et al. Sibship size, birth order, family structure and childhood mental disorders. Soc Psychiatry Psychiatr Epidemiol. 2013; 48: 1327-1333. Ref.: https://goo.gl/rRHbze
- Cohen J, Statistical power analysis for behavioural sciences. 1988, Hillsdale, NY: Lawrence Erlbaum Associates.
- StataCorp, Stata Statistical Software: Release 12. 2011, StataCorp LP: College Station, Texas.
- Hardt J. The Symptom-Check-List-27-plus (SCL-27-plus): A modern conceptualization of a traditional screening instrument. German Medical Science - Psychosoc Med. 2008; 5. Ref.: https://goo.gl/Uu7hWR
- Weyer L. Einzelkinder, Erstgeborene, Mittelgeborene und Letztgeborene: Langzeiteffekte des Geburtsstatus.
- In Deutschland und Polen. unveroeff. Dissertation, FB Medizin, Mainz. 2016.
- Wermuth N, Cox DR. On the relation between interactions obtained with alternative codings of discrete variables. Methodika. 1992; 6: 76-86.
- Hardt J, Bernert S, Matschinger H, Angermeier MC, Vilagut G, et al. Suicidality and its relationship with depression, alcohol disorders and childhood experiences of violence: results from the ESEMeD study. J Affect Disord. 2015; 175: 168-174. Ref.: https://goo.gl/JNYaf7
- Semler G, Wittchen HU, Joschke K, Zaudig M, von Geiso T, et al. Test-retest reliability of a standardized psychiatric interview (DIS/CIDI). Eur Arch Psychiatry Neurol Sci. 1987; 236: 214-222. Ref.: https://goo.gl/F2YzUk
- Statistisches Bundesamt. Demographie: Privathaushalte - Kinder und Einzelkinder unter 18.